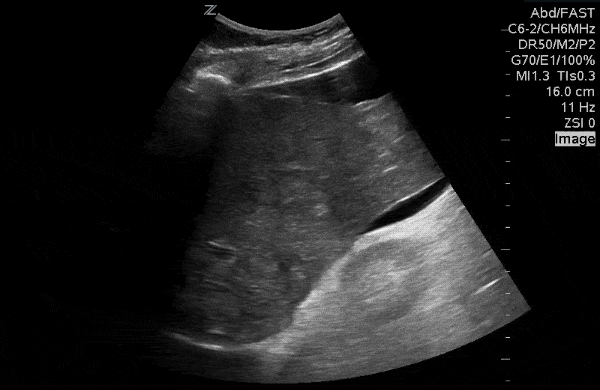
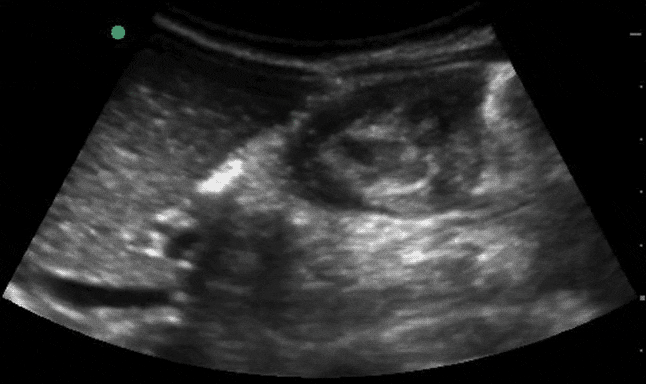
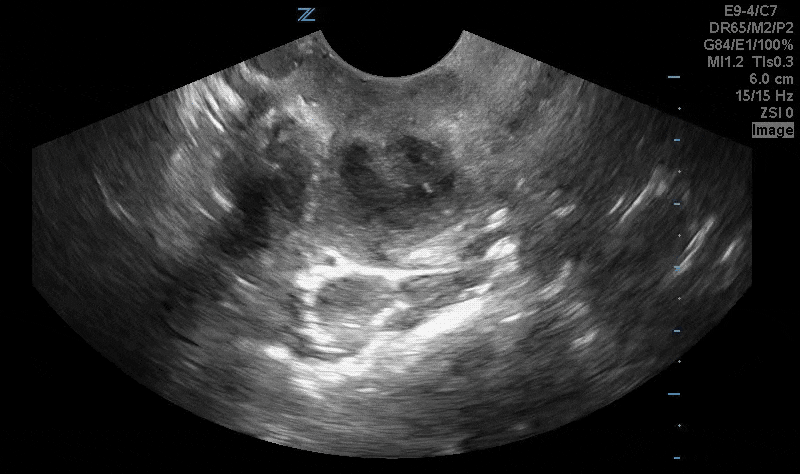
63yo M with fatigue and weight loss, generalized abdominal pain.

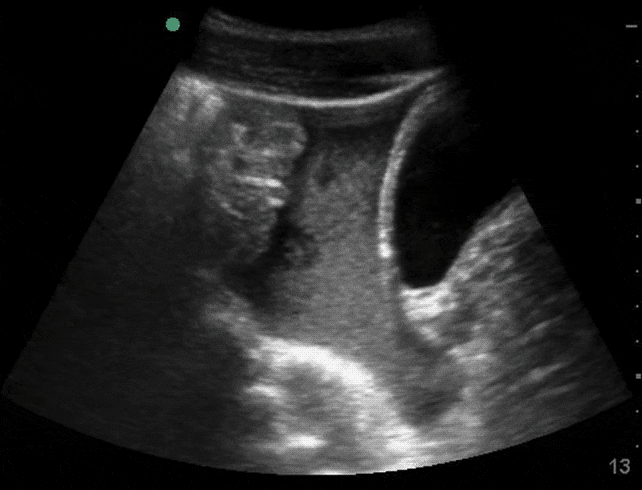
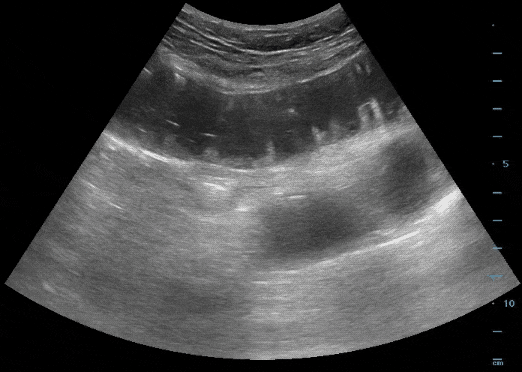
Renal ultrasound in setting of urinary retention.
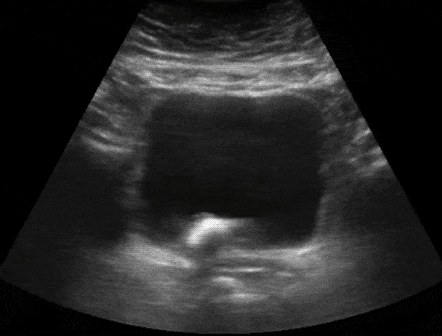
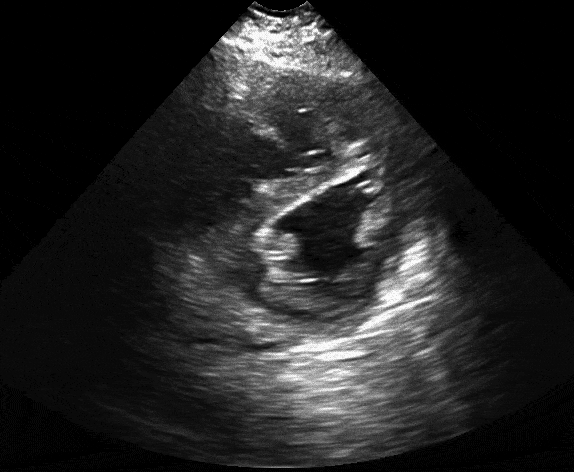
80yo M with bladder pain.
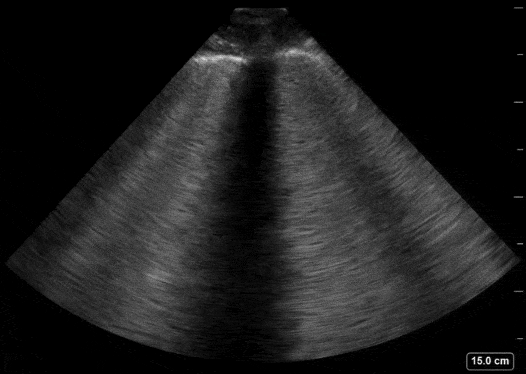
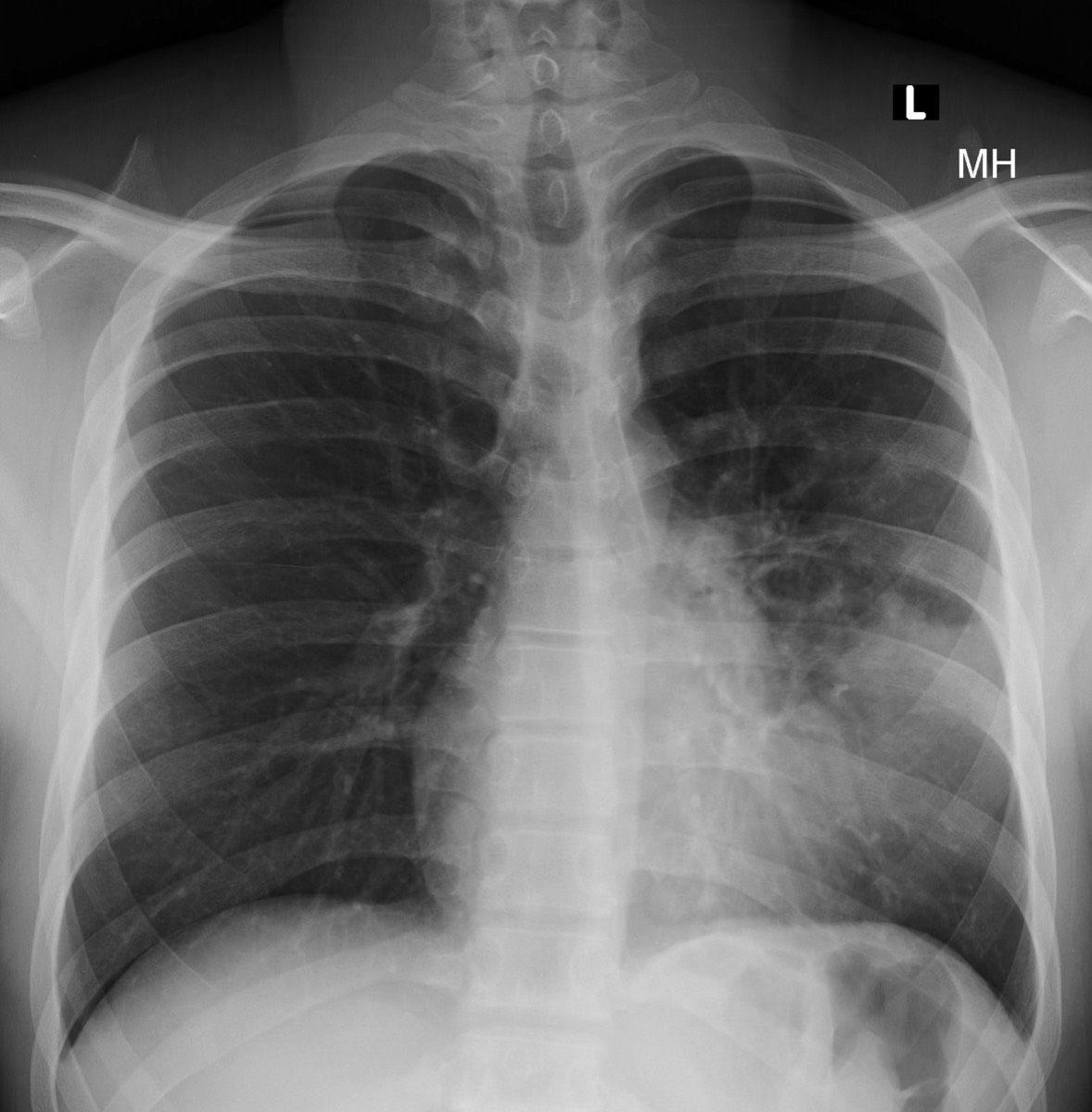
4yo with recent URI and shortness of breath.
4yo s/p "accidental" stab wound to chest.
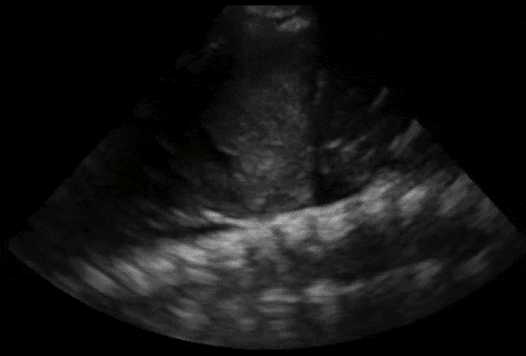
Describe the IVC.
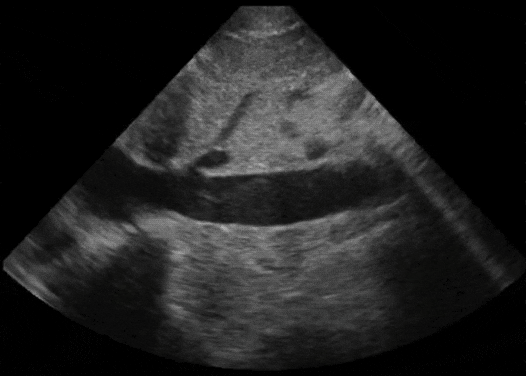
60yo M with progressive dyspnea and leg swelling.
Categorize the ejection fraction.
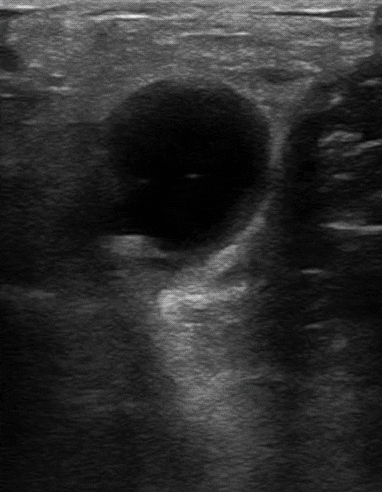
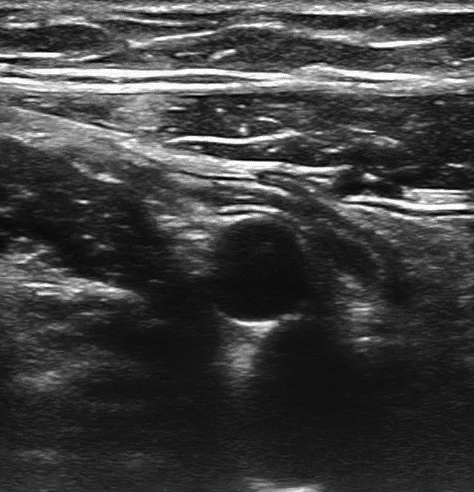
40yo F with calf pain and swelling. Imaging from the popliteal fossa.

Neck swelling and minimal pain to palpation. Anterior neck evaluation.
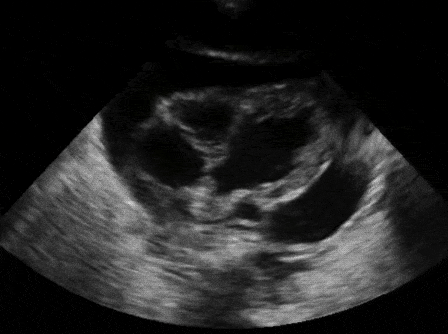
6yo M with RLQ pain. Operating room or home?

4yo with RLQ pain. Operating room or home?
12yo with a handlebar injury. Pelvic view in sagittal. Concerned?
14mo F with back arching and fussiness.

2yo with cough and fever. What is the sonographic finding?
24yo college student with a sore throat and enlarged tonsils. Is an aspiration indicated?

Sudden, painless vision loss.

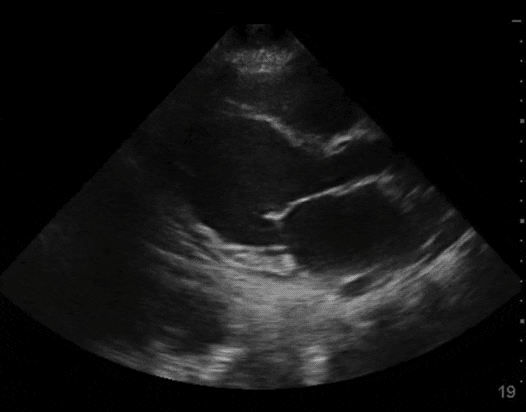
Decreased breath sounds at the lung base. Explanation?
Parasternal short axis with a pathologic finding.
Generalized abdominal pain. Frequent visits to the ED for gastroparesis.